
[:es]
Los avances de la microcirugía y de la supermicrocirugía han posibilitado el desarrollo de procedimiento quirúrgicos enfocados en mejorar el drenaje linfático. El objetivo de estos procedimientos en los casos de linfedema leve es lograr una extremidad normal que no necesite el uso de vendas o sistemas compresivos, y en los casos mas avanzados de linfedema el objetivo es disminuir el diámetro de la extremidad, disminuyendo o eliminando el riesgo de celulitis y de úlceras.
Dependiendo de la causa y grado del linfedema las opciones de cirugía más utilizadas son el trasplante de ganglios linfáticos y las anastomosis linfático-venosas.
En los casos leves de linfedema, donde es posible identificar vasos linfáticos sanos, se puede realizar la conexión de esos linfáticos directamente al sistema venoso en lo que se conoce como anastomosis linfático-venosa (LVA de su sigla en inglés). De esta forma se mejora el drenaje linfático de la extremidad o zona del cuerpo afectada.
El trasplante de ganglios (VLNT de su sigla en inglés) está especialmente indicado en casos moderados a severos de linfedema, donde muchas veces es difícil identificar vasos linfáticos sanos, y donde habitualmente la causa del linfedema ha sido la resección de ganglios linfáticos por cirugía oncológica. En esta cirugía se toman ganglios linfáticos sanos de forma cuidadosa de alguna parte del cuerpo para colocarlos en la extremidad afectada. Los ganglios trasplantados funcionan drenando directamente el linfedema al sistema venoso. De esta forma se mejora el drenaje linfático, disminuyendo el diámetro de la extremidad, la sensación de pesadez, el riesgo de complicaciones locales y la necesidad o la frecuencia de terapia kinésica especializada para drenaje linfático.
En algunos casos en necesario combinar el tratamiento de LVA con VLNT, y ayudar a la modelación de la extremidad con liposucción. En casos extremos es necesaria la resección de excedente cutáneo u otros procedimientos resectivos para disminuir el diámetro de la extremidad.
Trasplante de ganglios linfáticos
Para ver la entrevista en la página completa, puedes dar click en el siguiente enlace.
Realizan el primer trasplante de ganglios a un paciente con linfedema entrevista diario El Mercurio

En pie de guerra contra el linfedema
Microcirugía en Linfedema

Microcirugía en Linfedema Dr. Alejandro Ramírez
Microcirugía en Linfedema
La Microcirugía Reconstructiva es una de las herramientas más potentes para tratar el linfedema. Tanto la transferencia o trasplante de ganglios linfáticos así como las anastomosis linfático-venosas permiten mejorar de forma fisiológica el drenaje linfático.
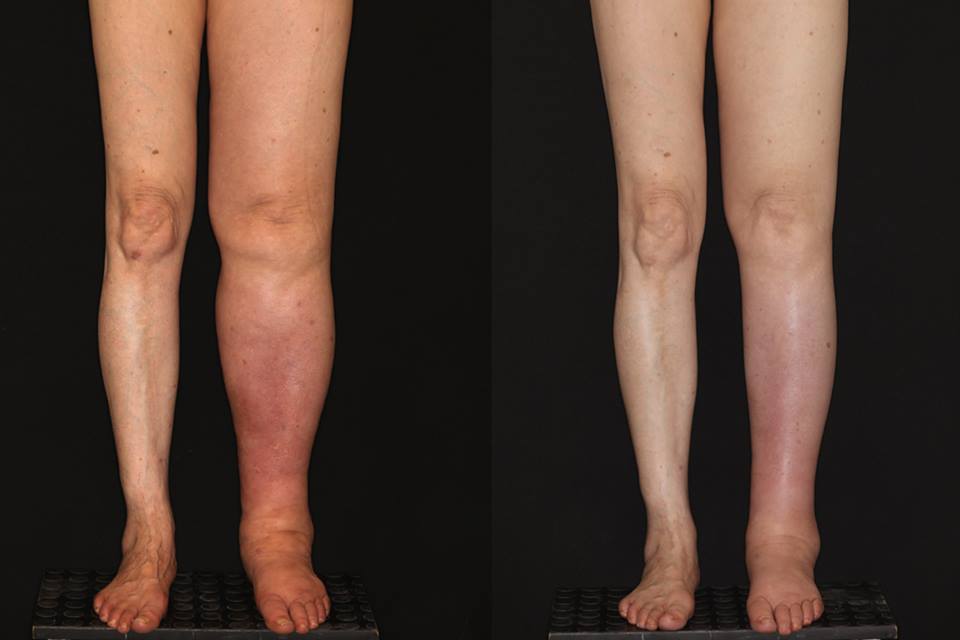
Les comparto el resultado a las 3 semanas en uno de nuestros pacientes. El fue sometido a disección ganglionar inguinal derecha como parte del tratamiento del cancer. Consultó con nosotros a los 7 meses por la aparición de linfedema de toda su extremidad inferior derecha. En este caso realizamos un trasplante de ganglios gastroepiploicos derechos a la ingle derecha. En la fotografía se puede observar la diferencia antes y después de la transferencia ganglionar.
Saludos,
Dr. Ramírez.
Tratamiento del Linfedema

Estamos muy contentos de poder ofrecer a nuestros pacientes con linfedema una nueva herramienta diagnóstica y que ayuda al tratamiento. Se trata del PDE, de la empresa japonesa Hamamatsu.
Tratamiento del linfedema:
Estamos muy contentos de poder ofrecer a nuestros pacientes con linfedema una nueva herramienta diagnóstica y que ayuda al tratamiento. Se trata del PDE, de la empresa japonesa Hamamatsu. Este sistema nos permite realizar la linfografía con verde de indocianina (ICG) para poder visualizar los vasos linfáticos y los distintos patrones de drenaje linfático. La linfografía con ICG nos permite optimizar el tratamiento ya sea con anastomosis linfático-venosas, trasplante de ganglios linfáticos o procedimientos resectivos como la liposucción o las resecciones directas.
Saludos,
Dr. Ramirez.
Microcirugía en linfedema: transferencia de ganglios linfáticos
La transferencia de ganglios linfáticos es una de las herramientas con que se cuenta actualmente para tratar de forma fisiológica el linfedema. Puede mejorar el contorno de la extremidad afectada, disminuir el riesgo de infecciones (celulitis) y otras complicaciones relacionadas con esta condición.
Les comparto un video resumen de una de las formas de realizar esta cirugía.
Saludos!
Primera Restauración Mamaria Total en Sudamérica

la mejor cirugia plastica estetica reconstuctiva
Equipo de Cirugía Plástica del HLF realiza primera Restauración Mamaria Anatómica Total en Sudamérica
El viernes 1 de julio en los pabellones de nuestro establecimiento se realizó una restauración mamaria anatómica total o TBAR, siendo esta la primera vez que se realiza esta intervención en nuestro País y en Sudamérica.
Dicha cirugía estuvo a cargo del equipo de Cirugía Plástica y Microcirugía Reconstructiva del HLF, liderado por el Dr. Alejandro Ramírez. La paciente intervenida fue una mujer de 56 años con cáncer de mama a la cual se le había realizado una mastectomía total y disección ganglionar axilar, secundario a la disección ganglionar, la Sra. Leonor Lagos, había evolucionado con linfedema (hinchazón por acumulación de linfa) en el brazo de ese mismo lado.En la compleja cirugía de 9 horas de duración, se realizó una reconstrucción mamaria con colgajo microquirúrgico DIEP, más un trasplante de ganglios linfáticos de la zona inguinal a la axila (TBAR).
La Sra. Leonor Lagos (primera paciente en ser intervenida de restauración mamaria anatómica total) junto a su hija Andrea Jiménez están felices con la operación.
El objetivo de esta cirugía fue tanto reconstruir la mama, como tratar el linfedema del brazo. Según explica el Dr. Ramírez, “la reconstrucción mamaria con colgajo DIEP es la mejor reconstrucción mamaria a la que las pacientes pueden optar, esto por que produce muy poco daño en la zona de donde se toma el tejido (siendo muy parecido a una abdominoplastía estética) y porque la mama reconstruida tiene un aspecto y consistencia natural”. Por otro lado, explica que “los ganglios linfáticos trasplantados cumplen su función succionando el linfedema y de esta forma mejoran el drenaje linfático de la extremidad afectada. Los beneficios del TBAR son poder reconstruir en una misma cirugía la mama afectada y el drenaje linfático del brazo”. El Dr. Ramírez recalca que la microcirugía para tratar el linfedema es un área de rápido desarrollo en el mundo gracias al progreso de la supermicrocirugía y del trasplante de ganglios linfáticos. “Con estas herramientas hoy podemos dar tratamiento a pacientes que antiguamente solo podían ser tratados con terapias kinesiológicas de drenaje linfático”.
La paciente no presentó complicaciones inmediatas y fue dada de alta el quinto día después de la cirugía.
El Dr. Alejandro Ramírez destacó el increíble trabajo realizado junto al equipo de Cirugía Plástica y microcirugía reconstructiva del HLF.
Te invito a ver el caso completo de la Sra. Leonor en el siguiente enlace.
ENTREVISTA: PRIMER TRASPLANTE DE GANGLIOS LINFÁTICOS PARA LINFEDEMA EN CHILE
Por Carlos Montes Z. Portal Multitemático Contenidos 123
A cargo del Cirujano Plástico de la Pontificia Universidad Católica, Microcirujano Reconstructivo formado en Taipei, con estudios en Cirugía Plástica Estética en Nueva York, don Alejandro Ramírez, se llevó a cabo el primer trasplante de ganglios linfáticos para linfedema en Chile.
Doctor, ¿qué nos puede decir de este primer trasplante en el país? ¿En qué consiste?
Respecto al procedimiento: El linfedema es una enfermedad debilitante para muchos pacientes. Consiste en la acumulación de linfa en alguna parte del cuerpo, habitualmente las extremidades. Efectivamente es primera vez que se realiza esta cirugía en el país. El objetivo de ésta es llevar ganglios sanos a donde hace falta. Estos funcionan “succionando” el linfedema. De esta forma se mejora es drenaje linfático de la extremidad afectada, disminuye su diámetro, y las molestias y los problemas asociados. En este caso puntual, la paciente sufre linfedema en su extremidad inferior derecha. Recibió tratamiento en el extranjero con respuesta parcial, por lo que se planificó un trasplante de ganglios. El 11 de marzo, en una cirugía de más de 9 horas se trasplantaron ganglios tomados de su axila izquierda a la ingle derecha. Para realizar el trasplante de tejido se reconectó bajo la visión de un microscopio una arteria, 2 venas y un canal linfático.
La honesta y crítica visión del paciente
Camila Sapag Sánchez, 22 años:
Cuéntanos tu experiencia con respecto al trasplante.
Bueno, la cirugía contó con un gran equipo médico. Una oncóloga, un cirujano plástico especializado en microcirugía, mi kinesióloga, anestesista, etc. Todos expertos en el manejo del tema. Básicamente monitorearon los ganglios de mi zona toráxica, sacando 3 de ellos sin riesgo de generar secuelas en la zona. Trasplantaron ese colgajo de 3 ganglios en mi zona inguinal derecha uniéndolos para mantenerlos vivos. Además de eso, me realizaron una liposucción en toda la extremidad para reducir el volumen. Es una cirugía lenta, que necesita mucha concentración y experticia porque son zonas delicadas, y la recuperación posterior es un poco dolorosa y lenta.
Al tratarse de ganglios linfáticos, ¿funciona con lista de espera, igual que un corazón o pulmón?
Es una transferencia ganglionar en donde se trasladan ganglios de la zona toráxica, lugar seguro sin riesgo de daño linfático, hacia otraparte del cuerpo, en mi caso la ingle. Como medida de prevención antes de la cirugía, es necesario realizar una linfocintigrafía para la marcación de ganglios mediante un líquido de contraste, el cual permite durante la cirugía monitorear que no se vean afectados los ganglios de la zona donde se extraen los ganglios para el trasplante. No funciona con lista de espera, sino que el trasplante se hace desde el propio cuerpo. En mi caso, me extrajeron un colgajo de 3 ganglios de la zona toráxica y los trasplantaron en la zona inguinal conectando los ganglios nuevos a arterias y venas. Además, en esa misma unión el doctor me realizó anastomosis.
¿Cómo contactaste al doctor que te operó?
Un día fui al centro médico El Golf a hacerme un drenaje linfático, donde trabaja mi kinesióloga experta en linfedema Angela Villella y ella me comentó que había llegado a Chile el doctor Alejandro Ramirez de la Universidad Católica. Se había ido un año a Taiwán a aprender la técnica del transplante de ganglios con expertos en el tema, entonces se nos abrió la posibilidad de contactarlo e implementar ese tipo de cirugía en Chile. Los especialistas en microcirugía reconstructiva son cirujanos plásticos, y el doctor Alejandro Ramirez nos dio confianza y seguridad con sus conocimientos y manejo del tema.
Antes de hacerlo, ¿había un plan B? Entiendo que tuviste que viajar fuera de Chile.
Mira, a mi me diagnosticaron Linfedema el año 2011. Llegué a la clínica a Urgencia pensando que me había picado un bicho o algo así porque desperté con la pierna derecha muy hinchada. Cuando me hice los
exámenes pertinentes, un doctor vascular me dio el diagnóstico, diciéndome que era una enfermedad para toda la vida, y que la única solución eran las medias de compresión, el drenaje manual y el vendaje multicapas. Me quedé con eso un par de años, resignada a mi condición hasta que con la ayuda de mi mamá, empezamos a descubrir que sí existían tratamientos alternativos, que sí existían opciones de mejorar la calidad de vida pero lamentablemente no en Chile y de muy alto costo. Nos comunicamos con Estados Unidos, Argentina, pero finalmente decidimos viajar a España donde nos acogieron muy bien, donde se nota el interés de los médicos y la inclusión de la patología en el servicio de salud. En España el doctor Lasso me hizo 5 anastomosis linfático- venosas (conectar vasos linfáticos a las venas) y obtuve una mejoría. Reduje la hinchazón de mi pierna, no del todo pero sí me alivió un montón y evitó que el volumen de mi pierna aumentara. Con eso, descubrimos también que no solo se puede realizar una sola intervención, sino que se puede intentar una, dos, tres veces incluso combinando técnicas.Es muy triste que en Chile el Linfedema no sea un tema que esté sobre la mesa de los temas médicos, porque un sinfín de mujeres que son víctima del cáncer de mamas terminan con Linfedema en un brazo, o yo en mi caso por una negligencia médica, debido a la biopsia de un ganglio inginal en la cual se produjo una extracción de una importante masa ganglionar sin tener las precauciones requeridas, produciendo obstrucción en el drenaje linfático; aún más, el resultado de la Biopsia no arrojó ninguna patología quedando el Linfedema como secuela de esta intervención. Los doctores en nuestro país no están informados de los avances que existen en el tratamiento de esta enfermedad y eso de cierta forma hace que los pacientes se condenen a una mala calidad de vida, se encierren en su condición y se sientan desesperanzados y solos. No sólo hay linfedemas secundarios, también hay linfedemas primarios que son congénitos. Mi caso es secundario, porque es producto de una mala manipulación de los ganglios en una biopsia.
Una vez recuperada, ¿vida normal?
Absolutamente. Dos semanas de reposo relativo, luego continuar con sesiones de drenaje linfático manual y vendajes multicapas pero con total movilidad y posibilidad de realizar una vida normal. Sí hay que decir que el Linfedema genera un grado de discapacidad porque imposibilita realizar ciertas actividades sobre todo cuando uno es joven. Osea, yo no puedo hacer mucho ejercicio de rebote, no puedo hacer caminatas muy largas porque se me inflama, y tengo que tener ciertas precauciones como no hacerme heridas, porque existen muchos riesgos que van de la mano del Linfedema. Por otro lado, siempre me he dicho a mi misma que no voy a cambiar por la enfermedad. Sí me adapto a ella pero en ningún grado he dejado de hacer las actividades que me gustan. Por ejemplo me voy a acampar un par de días donde sé que voy a realizar ejercicio físico y llevo mis vendas y mis cosas para cuidarme. Hay que aprender a incorporar esta enfermedad y no dejar que te paralice porque el efecto psicológico es fuerte. Las pacientes tienden a esconderse, a sentirse abandonadas, con la sentencia de que es una enfermedad progresiva que no tiene mejora y que finalmente produce mucho daño en la autoestima.
Para cerrar, ¿qué se siente ser parte de la historia médica del país?
Me parece relevante tener el privilegio de poder ser la cara visible que represente tantos casos silenciosos, ocultos, desprotegidos, ignorados, de personas que el día de mañana tendrán la oportunidad de mejorar su condición, de tener una vida más plena, feliz y que los médicos especialistas (vasculares, cirujanos plásticos y kinesiólogos) tomen conciencia y reaccionen frente a la necesidad de capacitarse, leer, asistir a congresos y hacerse cargo responsablemente de muchos pacientes que están a la espera de ser atendidos. También creo relevante insertar esta enfermedad en el sistema de salud, ya que no existe código Fonasa ni cobertura de isapre, y los tratamientos son de alto costo y sólo se pueden cubrir con recursos propios. En ese sentido, hay personas de escasos ingresos que no tienen posibilidades de atención. Yo espero que mi caso se difunda para que todas las personas que padecen Linfedema vean que sí hay alternativas, que sí existen médicos con voluntad de ayudar, que saben y se informan. Que sepan que el diagnóstico no es tan dramático como parece, que no están solos y que hay un millón de gente con la misma condición. En Facebook se creó un grupo que se llama Linfedema Acción, y es impresionante ver la cantidad de gente que tiene esta enfermedad y que no sabe cómo manejarla. Mis papás tienen los recursos para poder pagar los tratamientos, tengo la suerte de poder viajar a España, tengo la suerte de poder ahora tratarme en Chile, y quiero que toda la gente tenga esa misma suerte. Me parece insólito que el drenaje manual pase por algo estético y no lo cubra el servicio de salud, porque un drenaje linfático no es lo que hacen en los centros de estética, un drenaje linfático es una técnica médica que ayuda a mejorar la calidad de vida de personas agobiadas. No puede ser que sólo 30 kinesiólogos sean certificados en Drenaje Linfático con la cantidad de casos que existen en nuestro país. No puede ser que exista un mal manejo de ganglios en cualquier manipulación del cuerpo, porque los ganglios son fundamentales para todo el funcionamiento del cuerpo. No puede ser que uno vaya a una consulta médica y sepa más que el doctor de la enfermedad, eso es un claro reflejo de la ignorancia y de la poca importancia que se le da a esta patología en el país. Quiero ser parte de la historia médica pero no por los logros científicos, sino que por los logros humanos. Quiero que el trasplante de ganglios, las anastomosis y las distintas técnicas sean accesibles a cualquier persona de nuestro país, y no una oportunidad que esté mediada por la situación económica, porque no es justo. Estoy muy contenta del resultado de la cirugía, sin duda, pero quiero que esto sirva de apoyo para esta patología tan poco manejada en Chile, quiero facilitarle a las personas el contacto con profesionales que manejen y ayuden el tratamiento de la enfermedad, y sobre todo, quiero que el tratamiento sea de fácil acceso para mejorar la calidad de vida de miles de personas.
Entrevista: Primer Trasplante De Ganglios Linfáticos Para Linfedema En Chile

tratamiento linfedema dr alejandro ramirez Microcirugía en Linfedema
Microcirugía en Linfedema:
Muchas pacientes con mastectomía por cancer de mama, además de tener que lidiar con la reconstrucción de su mama, deben enfrentarse al linfedema de su brazo. Hoy existen opciones de prevención y tratamiento con las que antes no contábamos. La microcirugía nos permite mejorar el drenaje linfático de forma fisiológica.
Les quiero compartir el resultado al mes de seguimiento en una de nuestras paciente con TBAR (restauración mamaria anatómica total) (colgajo DIEP para reconstrucción mamaria más transferencia de ganglios linfáticos a la axila).
TRASPLANTE DE GANGLIOS PARA LINFEDEMA POR CANCER CERVICOUTERINO
Trasplante de ganglios para linfedema por cancer cervicouterino
Una de las complicaciones de la disección ganglionar por cancer cervicouterino es la aparición de linfedema en las extremidades inferiores. Afortunadamente existen opciones de tratamiento, como la transferencia ganglionar.
Este es el resultado en una de nuestras pacientes con linfedema, secundario a cancer cervicouterino. Tres meses después del trasplante ganglionar ha logrado un 70% de reducción del linfedema, mejorando enormemente su calidad de vida.
Tratamiento Integral Estético y Funcional del Linfedema:

Para mejorar el drenaje linfático en este caso realizamos un trasplante de ganglios linfáticos a la ingle derecha con Microcirugía
Este es el resultado en una de nuestras pacientes a un año de seguimiento. Para mejorar el drenaje linfático en este caso realizamos un trasplante de ganglios linfáticos a la ingle derecha con Microcirugía. Después de mejorado el drenaje linfático, en una segunda cirugía, realizamos liposucción circunferencial en 360º de la extremidad y lifting de muslo para tratar la hipertrofia grasa.
Nuestra paciente no ha vuelto a presentar episodios de celulitis, siente su pierna mucho más liviana, puede caminar sin problemas y esta muy contenta con el resultado estético.
The advances of microsurgery and supermicrosurgery have enabled the development of surgical procedures focused on improving lymphatic drainage. The objective of these procedures in cases of mild lymphedema is to achieve a normal limb that does not need the use of bandages or compression systems, and in the most advanced cases of lymphedema the objective is to decrease the diameter of the limb, decreasing or eliminating the risk of cellulitis and ulcers.
Depending on the cause and degree of lymphedema, the most commonly used surgery options are lymph node transplantation and lymphatic-venous anastomoses.
In mild cases of lymphedema, where it is possible to identify healthy lymphatic vessels, the connection of these lymphatics can be made directly to the venous system in what is known as lymphatic-venous anastomosis (LVA). In this way the lymphatic drainage of the affected limb or body area is improved.
Lymph node transplantation (VLNT) is especially indicated in moderate to severe cases of lymphedema, where it is often difficult to identify healthy lymphatic vessels, and where the cause of lymphedema has usually been the resection of lymph nodes. Oncological surgery lymph nodes. In this surgery, healthy lymph nodes are taken carefully from some part of the body to place them on the affected limb. The transplanted lymph nodes work by directly draining lymphedema into the venous system. In this way the lymphatic drainage is improved, decreasing the diameter of the limb, the sensation of heaviness, the risk of local complications and the need or frequency of specialized kinesic therapy for lymphatic drainage.
In some cases it is necessary to combine the treatment of LVA with VLNT, and to help the modeling of the limb with liposuction. In extreme cases it is necessary the resection of cutaneous surplus or other resective procedures to reduce the diameter of the limb.
Trasplante de ganglios linfáticos
Para ver la entrevista en la página completa, puedes dar click en el siguiente enlace.
On the warpath against lymphedema
Microcirugía en Linfedema
Lymphedema Microsurgery Dr. Alejandro Ramírez
Lymphoedema Microsurgery
Reconstructive Microsurgery is one of the most powerful tools to treat lymphedema. Both the transfer or transplantation of lymph nodes and the lymphatic-venous anastomoses allow a physiological improvement of the lymphatic drainage.
I share the result at 3 weeks in one of our patients. He underwent right inguinal lymph node dissection as part of the cancer treatment. He consulted us at 7 months due to the appearance of lymphedema of his entire lower right extremity. In this case, we performed a transplant of right gastroepiploic nodes to the right groin. In the photograph you can see the difference before and after the ganglion transfer.
Regards,
Dr. Ramírez.
Tratamiento del Linfedema
We are very happy to be able to offer our patients with lymphedema a new diagnostic tool that helps with treatment. This is the PDE, of the Japanese company Hamamatsu.
Lymphedema treatment:
We are very happy to be able to offer our patients with lymphedema a new diagnostic tool that helps with treatment. This is the PDE, of the Japanese company Hamamatsu. This system allows us to perform lymphography with indocyanine green (ICG) to visualize the lymphatic vessels and the different patterns of lymphatic drainage. Lymphography with ICG allows us to optimize treatment with either lymphatic-venous anastomosis, lymph node transplantation or resective procedures such as liposuction or direct resections.
Regards,
Dr. Ramirez.
Lymphedema microsurgery: lymph node transfer
The lymph node transfer is one of the tools that is currently available to treat lymphedema physiologically. It can improve the contour of the affected limb, decrease the risk of infections (cellulitis) and other complications related to this condition.
I share a video summary of one of the ways to perform this surgery.
Regards!
First Total Breast Restoration in South America
the best aesthetic reconstructive plastic surgery
HLF Plastic Surgery Team performs first Total Anatomical Breast Restoration in South America
On Friday, July 1, in the pavilions of our establishment, a total anatomical mammary restoration or TBAR was performed, this being the first time this intervention has been carried out in our country and in South America.
Said surgery was in charge of the team of Plastic Surgery and Reconstructive Microsurgery of the HLF, led by Dr. Alejandro Ramírez. The patient was a 56-year-old woman with breast cancer who had undergone a total mastectomy and axillary lymph node dissection, secondary to lymph node dissection, Mrs. Leonor Lagos, had evolved with lymphedema (swelling due to lymph accumulation) ) in the arm of that same side. In the complex surgery of 9 hours, a breast reconstruction with a DIEP microsurgical flap was performed, plus a lymph node transplant from the inguinal to the axilla (TBAR).
Mrs. Leonor Lagos (first patient to be operated on total anatomical breast restoration) with her daughter Andrea Jimenez are happy with the operation.
The goal of this surgery was both to rebuild the breast, and to treat lymphedema of the arm. According to Dr. Ramírez, «breast reconstruction with a DIEP flap is the best breast reconstruction that patients can choose, because it produces very little damage in the area where the tissue is taken (being very similar to a tummy tuck). aesthetic) and because the reconstructed breast has a natural appearance and consistency «. On the other hand, he explains that «the transplanted lymph nodes perform their function sucking the lymphedema and thus improve the lymphatic drainage of the affected limb. The benefits of TBAR are being able to reconstruct the affected breast and the lymphatic drainage of the arm in the same surgery «. Dr. Ramírez emphasizes that microsurgery to treat lymphedema is an area of rapid development in the world thanks to the progress of supermicrosurgery and lymph node transplantation. «With these tools we can now treat patients who in the past could only be treated with kinesiological lymphatic drainage therapies.»
The patient did not present immediate complications and was discharged on the fifth day after surgery.
Dr. Alejandro Ramírez highlighted the incredible work done with the team of Plastic Surgery and reconstructive microsurgery of the HLF.
I invite you to read the complete case of Mrs. Leonor in the following link.
HLF Plastic Surgery Team performs first Total Anatomical Breast Restoration in South America
INTERVIEW: FIRST TRANSPLANT OF LYMPHATIC GANGLIA FOR LINFEDEMA IN CHILE
By Carlos Montes Z. Portal Multitemático Contenidos 123
In charge of the Plastic Surgeon of the Pontifical Catholic University, Reconstructive Microsurgeon trained in Taipei, with studies in Aesthetic Plastic Surgery in New York, Mr. Alejandro Ramírez, the first lymph node transplant for lymphedema was carried out in Chile.
Doctor, what can you tell us about this first transplant in the country? What does it consist of?
Regarding the procedure: Lymphedema is a debilitating disease for many patients. It consists of the accumulation of lymph in some part of the body, usually the extremities. It is indeed the first time that this surgery is performed in the country. The goal of this is to bring healthy lymph nodes where needed. These work by «sucking» the lymphedema. In this way it is improved lymphatic drainage of the affected limb, decreases its diameter, and the discomfort and associated problems. In this specific case, the patient suffers from lymphedema in her right lower extremity. He received treatment abroad with partial response, so a lymph node transplant was planned. On March 11, in a surgery of more than 9 hours, nodes were transplanted from his left armpit to the right groin. To perform the tissue transplantation, an artery, 2 veins and a lymphatic channel were reconnected under the microscope.
In charge of the Plastic Surgeon of the Pontifical Catholic University, Reconstructive Microsurgeon trained in Taipei, with studies in Aesthetic Plastic Surgery in New York, Mr. Alejandro Ramírez, the first lymph node transplant for lymphedema was carried out in Chile.
Doctor, what can you tell us about this first transplant in the country? What does it consist of?
The honest and critical vision of the patient
Camila Sapag Sánchez, 22 years old:
Tell us about your experience with transplantation.
Well, the surgery had a great medical team. An oncologist, a plastic surgeon specialized in microsurgery, my kinesiologist, anesthetist, etc. All experts in the handling of the subject. Basically, they monitored the lymph nodes of my thoracic zone, removing 3 of them without risk of generating sequels in the area. They transplanted that flap of 3 nodes in my right inguinal area joining them to keep them alive. In addition to that, I had a liposuction on the entire limb to reduce the volume. It is a slow surgery, which needs a lot of concentration and expertise because they are delicate areas, and the subsequent recovery is a bit painful and slow.
When dealing with lymph nodes, does it work with a waiting list, like a heart or lung?
It is a ganglion transfer where lymph nodes move from the thoracic area, safe place without risk of lymphatic damage, to another part of the body, in my case the groin. As a preventive measure before surgery, it is necessary to perform a lymphocycintigraphy for the marking of nodes by means of a contrast fluid, which allows during the surgery to monitor that the lymph nodes of the area where the lymph nodes are removed for transplantation are not affected. . It does not work with waiting list, but the transplant is done from the body itself. In my case, I extracted a 3-node flap from the thoracic area and transplanted it into the inguinal area connecting the new ganglia to arteries and veins. In addition, in that same union the doctor performed anastomosis.
How did you contact the doctor who operated on you?
One day I went to the El Golf medical center to have a lymphatic drainage, where my expert lymphedema expert, Angela Villella, works and she told me that Dr. Alejandro Ramirez of the Catholic University had arrived in Chile. He had gone to Taiwan one year to learn the technique of lymph node transplantation with experts in the field, so we were able to contact him and implement this type of surgery in Chile. The specialists in reconstructive microsurgery are plastic surgeons, and Dr. Alejandro Ramirez gave us confidence and security with his knowledge and management of the subject.
Before doing so, was there a plan B? I understand that you had to travel outside of Chile.
Look, I was diagnosed with lymphoedema in 2011. I came to the clinic in Urgency thinking that I had been bitten by a bug or something because I woke up with my right leg swollen. When I did the
In the relevant examinations, a vascular doctor gave me the diagnosis, telling me that it was a lifelong disease, and that the only solution was compression stockings, manual drainage and multilayer bandaging. I stayed with that for a couple of years, resigned to my condition until with the help of my mother, we began to discover that there were alternative treatments, that there were options to improve the quality of life but unfortunately not in Chile and very high cost. We communicated with the United States, Argentina, but finally decided to travel to Spain where they welcomed us very well, where we can see the interest of the doctors and the inclusion of the pathology in the health service. In Spain, Dr. Lasso gave me 5 lymphatic-venous anastomoses (connecting lymphatic vessels to the veins) and I got an improvement. I reduced the swelling of my leg, not quite but it did relieve me a lot and prevented the volume of my leg from increasing. With that, we also discovered that not only can a single intervention be performed, but that one can try one, two, three times, even combining techniques. It is very sad that in Chile Lymphedema is not an issue that is on the table of topics doctors, because countless women who are victims of breast cancer end up with Lymphedema in one arm, or me in my case due to medical negligence, due to the biopsy of an ingrown ganglion in which there was an extraction of a large mass ganglionar without having the required precautions, producing obstruction in the lymphatic drainage; even more, the result of the Biopsy did not show any pathology, leaving Lymphoedema as a consequence of this intervention. The doctors in our country are not informed of the advances that exist in the treatment of this disease and that in a certain way causes patients to be condemned to a poor quality of life, to lock themselves in their condition and feel hopeless and alone. Not only are there secondary lymphedemas, there are also primary lymphedemas that are congenital. My case is secondary, because it is a product of poor manipulation of the lymph nodes in a biopsy.
Once recovered, normal life?
Absolutely. Two weeks of relative rest, then continue with sessions of manual lymphatic drainage and bandages multilayers but with full mobility and possibility of a normal life. Yes, it must be said that Lymphedema generates a degree of disability because it makes it impossible to perform certain activities, especially when one is young. I mean, I can’t do a lot of bouncing, I can not go for long walks because it’s inflamed, and I have to have certain precautions like not getting hurt, because there are many risks that go hand in hand with Lymphoedema. On the other hand, I’ve always told myself that I’m not going to change because of the disease. Yes I adapt to it but in no degree I have stopped doing the activities that I like. For example, I’m camping for a couple of days where I know I’m going to do physical exercise and take my bandages and my things to take care of myself. You have to learn to incorporate this disease and not let it paralyze you because the psychological effect is strong. Patients tend to hide, to feel abandoned, with the statement that it is a progressive disease that has no improvement and that ultimately produces much damage to self-esteem.
To close, how does it feel to be part of the medical history of the country?
It seems relevant to me to have the privilege of being the visible face that represents so many silent, hidden, unprotected, ignored cases of people who tomorrow will have the opportunity to improve their condition, to have a fuller, happier life and that medical specialists (vascular surgeons, plastic surgeons and kinesiologists) become aware and react to the need to train, read, attend conferences and responsibly take care of many patients who are waiting to be served. I also believe it is important to insert this disease into the health system, since there is no Fonasa code or isapre coverage, and the treatments are expensive and can only be covered with our own resources. In that sense, there are people of low income who do not have possibilities of attention. I hope that my case is disseminated so that all people suffering from lymphedema see that there are alternatives, that there are doctors willing to help, who know and are informed. Let them know that the diagnosis is not as dramatic as it seems, that they are not alone and that there are a million people with the same condition. On Facebook, a group called Lymphedema Action was created, and it is impressive to see how many people have this disease and do not know how to handle it. My parents have the resources to pay for the treatments, I am lucky to be able to travel to Spain, I am lucky to be able to treat myself in Chile now, and I want all the people to have the same luck. I find it unusual that the manual drainage goes through something aesthetic and not covered by the health service, because a lymphatic drainage is not what they do in aesthetic centers, a lymphatic drainage is a medical technique that helps improve the quality of life of people overwhelmed. It can not be that only 30 kinesiologists are certified in lymphatic drainage with the number of cases that exist in our country. It can not be that there is a bad management of ganglia in any manipulation of the body, because the ganglia are fundamental for the whole functioning of the body. It can not be that one goes to a medical consultation and knows more than the doctor of the disease, that is a clear reflection of the ignorance and of the little importance that is given to this pathology in the country. I want to be part of medical history but not for scientific achievements, but for human achievements. I want the lymph node transplant, the anastomosis and the different techniques to be accessible to any person in our country, and not an opportunity that is mediated by the economic situation, because it is not fair. I am very happy with the result of the surgery, without a doubt, but I want this to be a support for this pathology so little handled in Chile, I want to provide people with contact with professionals that manage and help the treatment of the disease, and above all , I want the treatment to be easily accessible to improve the quality of life of thousands of people.
Interview: First Lymph Node Transplantation for Lymphedema in Chile
treatment linfedema dr alejandro ramirez Microsurgery in Lymphoedema
Lymphedema Microsurgery:
Many patients with mastectomy for breast cancer, in addition to having to deal with the reconstruction of their breast, must confront the lymphedema of their arm. Today there are prevention and treatment options that we did not have before. Microsurgery allows us to improve lymphatic drainage physiologically.
I want to share the result with one month of follow-up in one of our patients with TBAR (total anatomical breast restoration) (DIEP flap for breast reconstruction plus lymph node transfer to the axilla).
GANGLIA TRANSPLANT FOR LYMPHEDEMA BY CERVIX CANCER
Lymph node transplant for cervical cancer
One of the complications of lymph node dissection due to cervical cancer is the appearance of lymphedema in the lower extremities. Fortunately, there are treatment options, such as ganglion transfer.
This is the result in one of our patients with lymphedema, secondary to cervical cancer. Three months after the lymph node transplant has achieved a 70% reduction in lymphedema, greatly improving their quality of life.
Integral Aesthetic and Functional Treatment of Lymphedema:
To improve the lymphatic drainage in this case we perform a transplant of lymph nodes to the right groin with Microsurgery
This is the result in one of our patients at one year of follow-up. To improve lymphatic drainage in this case we performed a lymph node transplant to the right groin with microsurgery. After improving lymphatic drainage, in a second surgery, we performed 360º circumferential liposuction of the limb and thigh lift to treat fat hypertrophy.
Our patient has not presented episodes of cellulitis, feels her leg much lighter, can walk without problems and is very happy with the aesthetic result.
[:zh]
显微外科手术和超级显微外科手术的进步使得发展专注于完善淋巴引流的外科手术疗程成为可能。在轻度淋巴水肿的案例中,这些疗程的目的是达到不需要使用绷带或加压系统的正常肢体,而对于较晚期的淋巴水肿的案例,其目标是减小肢体直径、减少或消除橘皮组织和溃疡的风险。
根据淋巴水肿的原因和等级,最常用的手术选择是淋巴结移植和淋巴静脉吻合手术。
在轻度淋巴水肿的案例,是可以识别出健康的淋巴管,这些淋巴管可以通过所谓的淋巴静脉吻合手术(英文缩写LVA)直接连接到静脉系统。这样一来,患肢或身体受影响部位的淋巴引流就会得到改善。
淋巴结移植(英文缩写VLNT)特别适用于中度至重度的淋巴水肿案例,在这种情况下通常很难识别出健康的淋巴管,并且淋巴水肿通常是由癌症手术切除淋巴结所引起的。在此手术中,健康的淋巴结要从身体的某个部位小心地取出并置在患肢上。被移植的淋巴结通过被淋巴水肿直接排入静脉系统而起作用。以此方式,改善了淋巴引流,减小了肢体的直径、沉重感、局部并发症的风险以及对淋巴引流进行专门的物理疗法的需要或频率。
在某些案例中,有必要将淋巴静脉吻合手术(LVA)与淋巴结移植(VLNT)结合使用,并通过吸脂手术帮助塑造肢体。在极端情况下,必须进行过多的皮肤切除或其他切除手术以减小肢体的直径。
Trasplante de ganglios linfáticos
Para ver la entrevista en la página completa, puedes dar click en el siguiente enlace.
Realizan el primer trasplante de ganglios a un paciente con linfedema entrevista diario El Mercurio
Este es un elemento de encabezado personalizado
我们必须对抗淋巴水肿的最有力武器之一是淋巴结转移。在此视频中,可以观察到置于前臂上的淋巴结转移,能够捕获淋巴并将其泵入静脉系统。作为对照,我们使用靛氰绿(荧光药物),将其注入到手部。
一个拥抱
Microcirugía en Linfedema
Microcirugía en Linfedema Dr. Alejandro Ramírez
淋巴水肿的显微外科
显微外科重建手术是治疗淋巴水肿的最强大工具之一。淋巴结的转移或移植以及淋巴静脉吻合均可以生理方式改善淋巴引流。
我向您分享其中一位患者的三周的术后结果。作为癌症治疗的一部分,患者接受了右腹股沟淋巴结切除手术。由于整个右下肢出现淋巴水肿,他在七个月后向我们咨询。在这种案例下,我们对右腹股沟进行了右胃表皮淋巴结移植。在照片中,您可以观察到淋巴结转移前后的差异。
Este es un elemento de encabezado personalizado
Estamos muy contentos de poder ofrecer a nuestros pacientes con linfedema una nueva herramienta diagnóstica y que ayuda al tratamiento. Se trata del PDE, de la empresa japonesa Hamamatsu.
淋巴水肿治疗
我们很高兴能够为淋巴水肿患者提供一种新的诊断和治疗辅助工具。它是日本滨松光子学株式会社(Hamamatsu)的光子探测效率(PDE)。该系统使我们能够执行靛氰绿淋巴造影(ICG),以可视化淋巴管和淋巴引流的不同模式。ICG淋巴造影使我们能够优化治疗,无论是淋巴静脉吻合术、淋巴结移植还是切除手术(例如吸脂或直接切除手术)。
Este es un elemento de encabezado personalizado
淋巴结转移是目前可用于生理学治疗淋巴水肿的工具之一。它可以改善患肢的轮廓、降低感染(蜂窝组织炎)和与此疾病相关的其他并发症的风险。
我向您分享了执行该手术方法之一的视频摘要。
Primera Restauración Mamaria Total en Sudamérica
la mejor cirugia plastica estetica reconstuctiva
HLF整形外科团队在南美洲进行了首例全面解剖乳房修复
7月1日星期五,在我们医院的外科病房内进行了全面解剖乳房修复(TBAR),这是在我们的国家(智利)和南美洲首次进行这种手术。
该手术是由亚历山大·拉米雷斯(AlejandroRamírez)医师领导的HLF整形外科和显微外科重建团队负责。接受手术的患者是一名56岁的乳腺癌女性,曾接受全乳房切除手术和腋窝淋巴结切除手术,继之以淋巴结切除手术,莱昂纳尔·拉各斯女士(Leonor Lagos)在同一侧的手臂上演变为淋巴水肿(由于淋巴积聚而肿胀)。在九个小时的复杂手术中,使用显微外科皮瓣手术(DIEP)进行了乳房重建(TBAR),并从腹股沟区到腋窝进行了淋巴结移植。
莱昂纳尔·拉各斯女士(Leonor Lagos)(第一位接受全面解剖乳房修复手术的患者)和其女儿安德烈雅·西梅奈斯(Andrea Jiménez)女士对该手术感到满意。
该手术的目的是重建乳房并治疗手臂的淋巴水肿。如拉米雷斯医师(Dr.Ramírez)所述:“ DIEP皮瓣乳房重建手术是患者可以选择的最佳乳房重建手术,这是因为它在组织切除部位几乎不产生损伤(与腹部美容整形手术非常相似),因为重建的乳房具有自然的外观和稳定性”。
另一方面,他解释说:“移植的淋巴结通过吮吸淋巴水肿来发挥其功能,从而改善患肢的淋巴引流。全面解剖乳房修复(TBAR)的优点是能够在同一手术中重建受影响的乳房和手臂的淋巴引流”。拉米雷斯医师(Dr.Ramírez)强调说,由于超级显微手术和淋巴结移植的进步,用于治疗淋巴水肿的显微外科手术是全世界一个快速发展的领域。“有了这些工具,今天我们可以治疗在以前只能用淋巴引流物理治疗法治疗的患者。”
该患者无立即并发症,手术后第五天出院。
亚历山大·拉米雷斯医师(Dr. Alejandro Ramírez)强调了与HLF整形外科和显微外科重建团队一起开展的不可思议的手术。
我邀请您在以下链接中查看莱昂纳尔·拉各斯女士(Leonor Lagos)的完整案例。
ENTREVISTA: PRIMER TRASPLANTE DE GANGLIOS LINFÁTICOS PARA LINFEDEMA EN CHILE
Por Carlos Montes Z. Portal Multitemático Contenidos 123
访谈文章:智利首次淋巴水肿的淋巴结移植
作者:卡洛斯•蒙特(Carlos Montes Z)的多主题门户内容123
身为智利天主教大学(Pontificia Universidad Católica)整形外科负责人,在台北接受培训成为显微重建外科医师,并在纽约进行了美容整形外科研究,亚历山大•拉米雷斯医师(Alejandro Ramírez)在智利进行了首例用于淋巴水肿的淋巴结移植手术。
医生,您能告诉我们关于本国(智利)的第一次移植手术吗?它是由什么组成?
关于手术:淋巴水肿对于许多患者是一种虚弱疾病。它由身体某些部位(通常是四肢)的淋巴液积累组成。的确,这是本国(智利)第一次进行这种手术。手术目的是在让需要它们的地方获得健康淋巴结。通过“吮吸”淋巴水肿可起作用。这样一来,患肢的淋巴引流得到改善,其直径大小、不适感和问题就减少了。在这种特定案例下,患者右下肢患有淋巴水肿。她在国外接受了局部治疗,因此计划进行淋巴结移植。3月11日,经过长达9个小时的手术,移植了从左腋窝到右腹股沟的淋巴结。为了进行组织移植,在显微镜的观察下重新连接了一条动脉、两条静脉和一条淋巴通道。
患者的诚实和批判性眼光
卡米拉·萨帕格·桑切斯小姐(Camila SapagSánchez),22岁:
请告诉我们,您在接受移植手术的经验。
好的,手术方面有个很棒的医疗团队,肿瘤科医生、专门从事显微外科的整形外科医生、我的物理治疗师、麻醉师等。有处理移植主题的所有专家。基本上他们监测了我胸腔区域的淋巴结,取出了其中的三个淋巴结,同时没有在胸腔区域产生后遗症的风险。他们将三个淋巴结皮瓣移植到我的右腹股沟区域,将它们连接起来以保持其活跃。除此之外,我还进行了全肢吸脂手术以减少水肿体积。这是一种缓慢的手术,因为它们是脆弱的区域,因此需要全神专注和大量专业知识,并且术后恢复有些痛楚且缓慢。
关于淋巴结移植手术,它是否像心脏或肺一样,需要等待移植才能进行呢?
这是淋巴结转移,来自胸部区域的淋巴结被转移到身体的另一部分,在我的案例是腹股沟,这是一个安全的地方,没有淋巴损伤的风险。作为外科手术前的预防措施,有必要使用造影剂对患者的淋巴组织进行淋巴造影检查,这可以在手术过程中监测为了移植淋巴结而被移除区域的淋巴结沒有受到影响。不用等待移植才能进行,而是移植是从身体本身进行的。以我为例,医师从我胸腔区域切除了三个淋巴结皮瓣,然后将它们移植到腹股沟区,将新淋巴结连接到动脉和静脉。此外,在同一连接处,医生对我进行了吻合手术。
您是如何联系上对您进行手术的医生的?
有一天,我去了埃尔高尔夫(El Golf)医疗中心进行淋巴引流,我的物理治疗师、淋巴水肿专家安琪拉•维耶雅医师(Angela Villella)在那里工作,她告诉我,天主教大学(Universidad Católica)的亚历山大•拉米雷斯医师(Alejandro Ramírez)到达了智利。他去台湾学习了一年,与当地有关专家学习了淋巴结移植技术,于是与他联系后,在智利实施该手术的可能性为我们打开了一扇大门。显微外科重建的专家是整形外科医生,亚历山大•拉米雷斯医师(Alejandro Ramírez)凭借着他对这手术了解和掌握,给了我们信心和安全感。
在进行手术之前,有没有计划B?我知道您必须去智利以外的地方旅行。
是这样的,我在2011年被诊断出淋巴水肿。我来到医院急诊室以为自己被虫子或类似东西咬伤了,因为我醒来时右腿非常肿胀。当我完成相关检查后,一位血管医师给了我诊断,告诉我这是我终其一生的疾病,唯一的解决方法是压力弹性袜、手动引流和多层绷带。这种方式持续了几年后我放弃了,在母亲的帮助下,我们开始发现确实存在替代疗法,确实存在着提高生活质量的选择,但不幸的是,在智利并没有,并且十分昂贵。我们曾与美国、阿根廷联系过,但最终我们决定前往西班牙,在那里他们非常欢迎我们,那边医师们的热忱以及将病理学纳入卫生服务的情况引人注目。在西班牙,拉索医师对我(Lasso)进行了5次淋巴静脉吻合术(将淋巴管连接到静脉),我得到了改善。手术减轻了我的腿部肿胀,没有完全消除,但确实给了我很多缓解,并防止了我的腿继续肿大。这样一来,我们还发现不仅只可以进行一次手术,甚至可以结合技术尝试一次、两次、三次。令人遗憾的是,在智利淋巴水肿并不受到医疗问题的关注,因为有无数个罹患乳腺癌的妇女在单臂患上淋巴水肿,或者在我的情况下,是由于医疗疏忽导致的腹股沟淋巴结活检,其中切除了重要淋巴结肿块而并未采取必要的预防措施,导致淋巴引流阻塞;此外,活检的结果未显示任何病理,留下淋巴水肿是该手术的后遗症。我们国家(智利)的医师并不了解存在于该疾病的治疗进展,并且以某种方式使患者谴责自己不佳的生活质量,他们将自己封闭在自己的状况中,感到绝望和孤独。不仅有继发性淋巴水肿,也有先天性原发性淋巴水肿。我的病例是继发性的,因为它是在活检中对淋巴结的操作不良而导致。
当恢复后,生活正常了吗?
绝对是的。相对休息两周,然后继续进行手动淋巴引流和多层绷带治疗,但活动能力完全正常,并可以正常生活。必须说,淋巴水肿会造成一定程度的残疾,因为它让我无法进行某些活动,尤其对于一个年轻人而言。我的意思是说,我不能做太多的弹跳运动、我不能走很长的路,因为我会发炎,而且我必须采取某些预防措施,例如尽量避免受伤,因为手部淋巴水肿存在很多风险。另一方面,我始终告诉自己,我不会因为这种疾病而改变。我确实适应了它,但是我丝毫没有停止做自己喜欢的活动。例如,我要去露营几天,在那里我知道我要进行体能锻炼,我带着绷带和物品照顾自己。必须要学会与这种疾病合为一体,而不能因它而停下,因为心理影响是很强烈的。患者倾向于躲藏起来,感到被抛弃,认为这是一种渐进性疾病,不可能有好转,最终导致自尊心受到很大损害。
最后,成为国家医疗史的一部分,感觉如何?
对我来说是意义非凡的,有幸能够被大家看见,代表了许多沉默、隐藏、不受保护、被忽视的案件,在明天的他们将机会改善自己的状况,过着更充实、更幸福的生活。希望专业医师(血管、整形外科医师和物理治疗师)更意识到并响应自我培训、阅读,参加会议的需要,并对许多等待护理的患者负起责任。我也认为将这种疾病列入医疗系统是十分重要的,因为没有国家健康基金(Fonasa)的代码或是社会保障机构(Isapre)的保险,治疗费用昂贵并且只能用自己的钱来支付。因此,有些低收入者没有受到护理的可能性。我希望我的案例能传播出去,让所有患有淋巴水肿的人都能知道有替代疗法,要知道有愿意帮助的医生。让他们知道,诊断并不像看起来那样戏剧性,他们并不孤单,有相当多人患有同样的疾病。在脸书Facebook上创建了一个名为“淋巴水肿行动”的群組,出人意表的看到有相当多人有这种疾病并且不知道如何处理。我的父母有足够的资源来支付治疗费用,我很幸运能够去西班牙旅行,我很幸运现在能够在智利自我治疗,我希望所有人都拥有同样的好运。在我看来,人工引流是通过美学方式进行的,并且不属于医疗保险范围之内,这是不正常的,因为淋巴引流不是美容中心所要进行的,淋巴引流是一种有助于改善不堪重负的人生活质量的医疗技术。只有30名获得淋巴引流证书的物理治疗师,来护理本国(智利)存在的所有案件患者,这是不可能的。人体的任何操纵中存在着淋巴结的不良掌控,这是不可能的,因为淋巴结对于身体的性能至关重要。某人去到医院但是却比医师更了解病情,这是不可能的,这清楚地反映了无知和对本国(智利)病理学的不重视。我想成为医学史的一部分,但不是因为科学成就,而是因为人性成就。我希望我们国家的任何人都可以接受淋巴结移植手术、吻合手术和其他各种手术技术,而不是经济状况所带来的一个机会,因为这是不公平的。毫无疑问,我对术后结果感到非常满意,但是我希望这可以为这种病理学提供支持,而这种病理学在智利受到很少的掌控,我想促进于患者与善于掌控和帮助治疗该疾病的专业医师之间的联系,尤其是,我希望可以轻松获得治疗以改善数千人的生活质量。
Entrevista: Primer Trasplante De Ganglios Linfáticos Para Linfedema En Chile
访谈文章:智利首次进行淋巴水肿的淋巴结移植
Entrevista: Primer Trasplante De Ganglios Linfáticos Para Linfedema En Chile
tratamiento linfedema dr alejandro ramirez Microcirugía en Linfedema
淋巴水肿的显微外科手术:
许多因乳腺癌而接受乳房切除手术的患者,除了必须处理乳房重建以外,还必须面临手臂的淋巴水肿。今天,已存在着过去没有的预防和治疗选择。显微外科手术使我们能够以生理方式改善淋巴引流。
我想与您分享我们的一名全面解剖乳房修复(TBAR)(用于乳房重建DIEP皮瓣以及淋巴结转移到腋窝)的患者在一个月的追踪后的术后结果。
淋巴结移植治疗子宫颈癌引发的淋巴水肿
Trasplante de ganglios para linfedema por cancer cervicouterino
子宫颈癌淋巴结切除的并发症之一是出现下肢淋巴水肿。幸运的是,有多种治疗选择,例如淋巴结转移。
这是其中一名患有子宫颈癌的淋巴水肿患者的术后结果。淋巴结移植三个月后,患者的淋巴水肿减少了70%,极大地改善了她的生活质量。
淋巴水肿的美学和功能综合治疗:
Para mejorar el drenaje linfático en este caso realizamos un trasplante de ganglios linfáticos a la ingle derecha con Microcirugía
为了改善淋巴引流,在这种病例中,我们通过显微外科手术将淋巴结移植到右腹股沟。
这是其中一位患者接受一年随访的结果。为了改善这种案例的淋巴引流,我们通过显微外科手术将淋巴结移植到右腹股沟。改善淋巴引流后,在第二次手术时,我们进行了360度肢体的环形吸脂手术和大腿提拉手术,以治疗脂肪肥大。患者没有再出现橘皮组织发作,腿部感觉更轻,可以行走没有问题,并且对美学效果感到非常满意。[:]